PathologyRadiologyOmicsLabsClinical
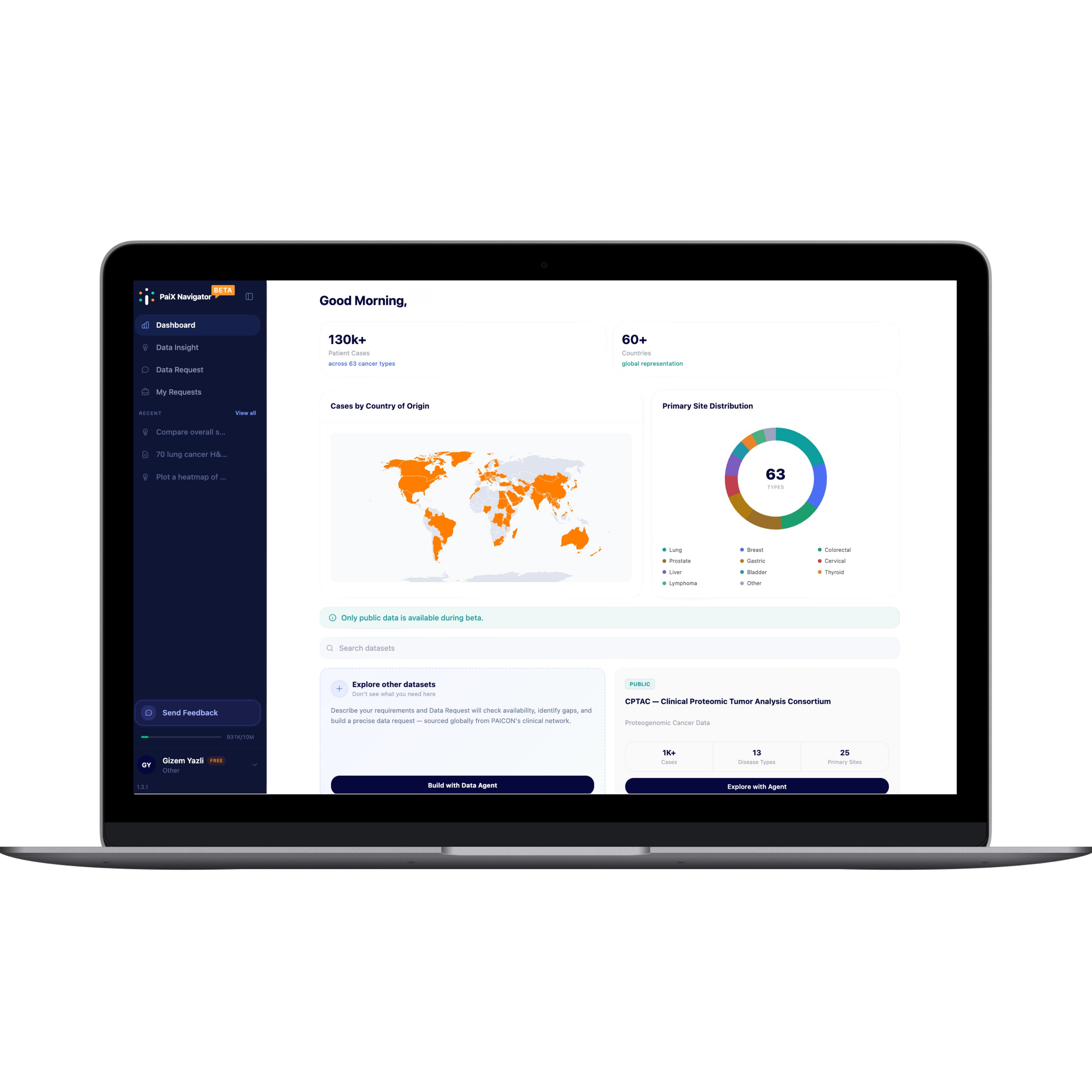
Multi-Modal Global Data
Pathology & clinical live now. More on the way.
Pathology and clinical data are available in PaiX Navigator today; radiology, omics and labs are coming soon, all harmonized end to end across 60+ countries.